
Bodybuilding
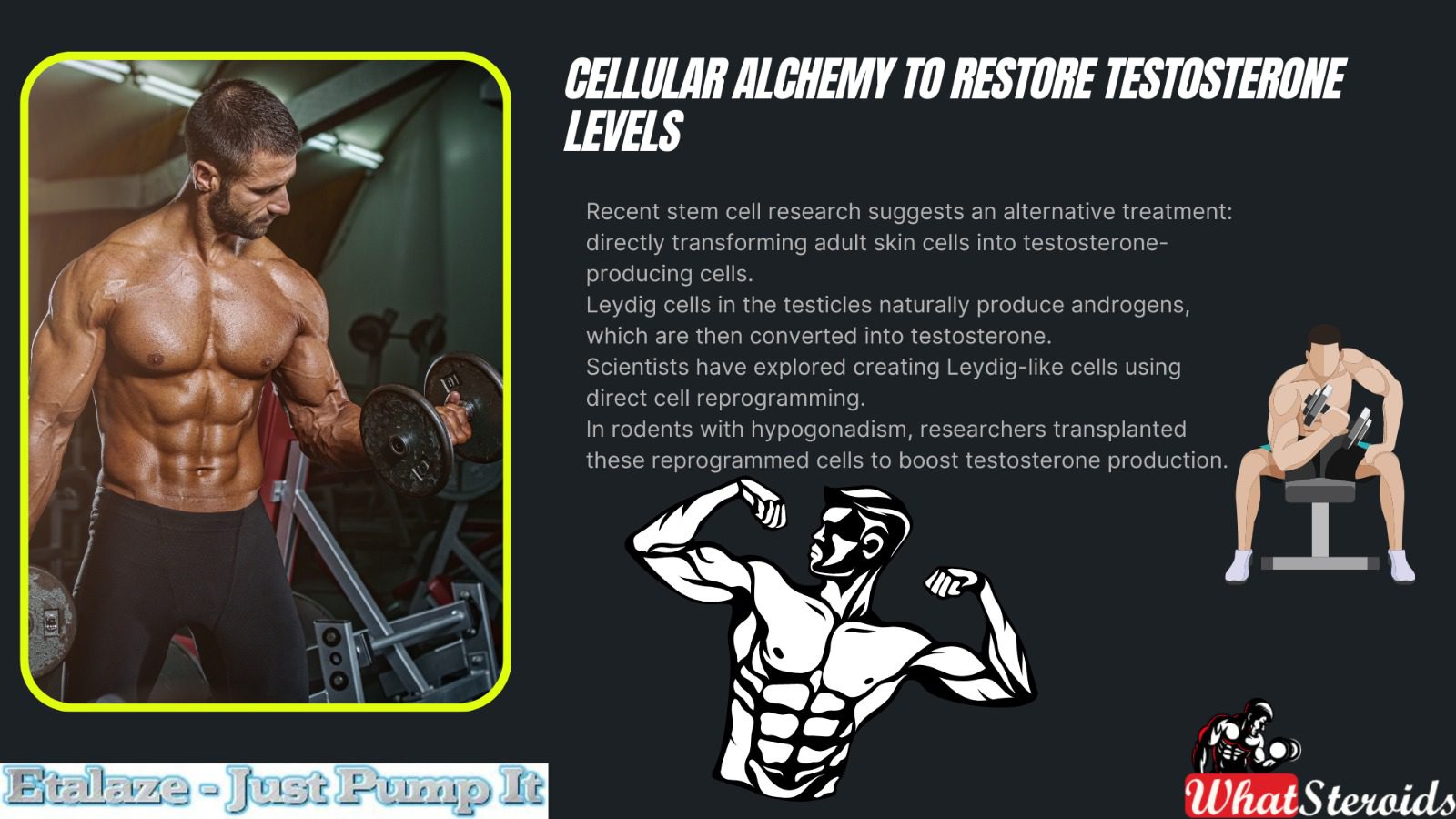
Cellular Alchemy to Restore Testosterone Levels
The convergence of stem cell therapy and hormone regulation represents an intriguing frontier in medical research, especially regarding the possibility of enhancing testosterone levels. In this article, we shall explore cellular Alchemy from a bodybuilding perspective.
Anabolic testosterone, the essential male hormone, plays a crucial role in various bodily functions, including muscle mass maintenance, bone density, and mood regulation. As men age, natural declines in testosterone levels can lead to hypogonadism, significantly affecting their quality of life.

Stem cell therapy or cellular Alchemy offers a promising avenue for restoring testosterone levels, even in bodybuilders. Let’s delve into the details:
Background on Testosterone and Hypogonadism
Testosterone is crucial for male sexual development, cognitive function, and overall health.
As men age, testosterone levels naturally decline, leading to conditions like hypogonadism (abnormally low testosterone).
Hypogonadism can cause mood disturbances, reduced sex drive, and weakened muscle and bone strength.
Traditional Approach: Testosterone Replacement Therapy (TRT)
The common clinical approach is anabolic testosterone replacement therapy (TRT).
However, TRT has significant side effects, including venous thromboembolism and deep vein thrombosis.
Stem Cell Research and Alternative Treatment
Recent stem cell research suggests an alternative treatment: directly transforming adult skin cells into testosterone-producing cells.
Leydig cells in the testicles naturally produce androgens, which are then converted into testosterone.
Scientists have explored creating Leydig-like cells using direct cell reprogramming.
In rodents with hypogonadism, researchers transplanted these reprogrammed cells to boost testosterone production.
Must Read: Muscle Disorders: Diagnosis, Treatment and Coping Routine
Implications for Bodybuilders
Stem cell therapy could benefit bodybuilders by:
Enhancing muscle growth: Stem cells may stimulate muscle repair and regeneration.
Improving recovery: Faster recovery after intense workouts.
Alleviating symptoms: Reduced libido, fatigue, and muscle loss associated with low testosterone.
Stem cell therapy for testosterone restoration is an exciting field, but it’s essential to understand both its potential benefits and risks. Let’s explore:
Testosterone Replacement Therapy (TRT) Risks
TRT is the common clinical approach for hypogonadism (low testosterone).
However, TRT has notable side effects, including:
Increased risk of blood clots: TRT can lead to elevated red blood cell production, potentially causing blood clots.
Sleep apnea risk: Some individuals on TRT may experience interrupted breathing during sleep.
Testicular atrophy: The testicles may shrink due to TRT.
Prostate growth: Regular prostate cancer monitoring becomes necessary.
Stem Cell Therapy Approach
Recent research explores an alternative: directly transforming adult skin cells into anabolic testosterone-producing cells.
Scientists aim to create Leydig-like cells using direct cell reprogramming.
Leydig cells in the testicles naturally produce androgens, which then convert into testosterone.
In rodent studies, researchers transplanted these reprogrammed cells to boost testosterone production2.
Implications and Caution
Stem cell therapy shows promise, but it’s still experimental.
Risks associated with stem cell therapy are not fully understood.
Safety, efficacy, and long-term effects need further investigation.
Cellular Alchemy Success Rate
Stem cell therapy for anabolic testosterone restoration shows promising results, particularly in the context of male hypogonadism. Let’s explore the success rates based on recent research:
Background on Male Hypogonadism
Male hypogonadism is characterized by abnormally low testosterone levels.
It can lead to mood disturbances, reduced sex drive, and decreased muscle and bone strength.
Approximately 30% of older men are affected by this condition.
Common Clinical Approach: Testosterone Replacement Therapy (TRT)
TRT is the standard treatment for hypogonadism.
However, TRT has significant side effects, including venous thromboembolism and deep vein thrombosis.
Stem Cell Research and Leydig-Like Cells
Scientists have explored an alternative using stem cells.
They directly transform adult skin cells into Leydig-like cells, which produce androgens and then biosynthesize testosterone.
In rodent studies, these reprogrammed Leydig cells were transplanted into testosterone-deficient animals.
Remarkably, the cells survived and restored normal testosterone levels in males with hypogonadism.
Success Rate
While individual outcomes may vary, stem cell therapy has shown promise.
Success rates are not universally defined, but the approach offers an exciting alternative to androgen replacement therapy.
Related Article: First Injectable Steroid Cycle
Holistic Approach to Men’s Health
Research Progress: As scientific knowledge advances, we recognize that health interventions should consider the whole person, not just isolated aspects.
Stem Cell Therapy: This emerging field offers potential benefits for various health conditions, including hypogonadism (low testosterone).
Holistic View: Rather than focusing solely on stem cell therapy, we should integrate it into a broader approach that considers lifestyle factors.
Lifestyle Factors and Testosterone
Diet: Proper nutrition is crucial. Certain nutrients (like zinc and vitamin D) support testosterone production.
Exercise: Regular physical activity, especially resistance training, positively influences testosterone levels.
Stress Management: Chronic stress can lower testosterone. Techniques like meditation and relaxation help maintain hormonal balance.
Complementary Role of Stem Cell Therapy
Enhancing Well-Being: Stem cell therapy complements lifestyle efforts.
Managing Hypogonadism: It can address anabolic testosterone deficiency, but it’s not a standalone solution.
Synergy: Combining stem cell therapy with lifestyle changes creates a comprehensive strategy.
Overall Health: This approach benefits not only testosterone levels but also overall health and vitality.
Viewing stem cell therapy holistically involves integrating it with lifestyle choices, creating a synergistic approach to men’s health.
Dietary Recommendations to Support Cellular Alchemy
 Buy Cabaser 1 mg [20 Tabs, Pfizer]
Buy Cabaser 1 mg [20 Tabs, Pfizer]
When it comes to managing hypogonadism, dietary choices play a crucial role. Here are some dietary recommendations:
Nutrient-Rich Foods
Zinc: Include foods like oysters, beef, pumpkin seeds, and legumes. Zinc supports testosterone production.
Vitamin D: Fatty fish (salmon, mackerel), fortified dairy products, and sunlight exposure help maintain healthy levels.
Healthy Fats: Avocado, nuts, and olive oil provide essential fats for hormone synthesis.
Avoid Excessive Alcohol and Sugar
Alcohol can negatively impact testosterone levels.
High sugar intake may lead to insulin resistance, affecting hormonal balance.
Protein Intake
Adequate protein supports muscle growth and overall health.
Include lean meats, eggs, and plant-based protein sources.
Anti-Inflammatory Foods
Chronic inflammation can affect testosterone.
Consume fruits, vegetables, and whole grains to reduce inflammation.
Natural Alternatives to Cellular Alchemy
If you’re looking for natural ways to boost anabolic testosterone without relying on cellular alchemy, consider the following strategies:
Ashwagandha Supplement
Ashwagandha, an adaptogenic herb, has been linked to reduced stress and increased testosterone levels.
In studies, it improved muscle strength and testosterone in men who took 600 mg daily for eight weeks.
Note that it didn’t have the same effect on women.
Prioritize Sleep
Aim for 7-9 hours of quality sleep each night.
Lack of sleep can lower testosterone levels, so prioritize rest.
Optimize Vitamin D
Vitamin D deficiency is associated with low testosterone.
Get sunlight exposure or consider supplements if needed.
Dietary Choices
Certain foods can help raise testosterone:
Grass-fed beef: Rich in nutrients and healthy fats.
Zinc-rich foods: Oysters, beef, and pumpkin seeds.
Vitamin D sources: Fatty fish and fortified dairy products.
Keep in mind that a holistic approach that combines lifestyle changes, nutrition, and natural supplements can contribute to maintaining healthy anabolic testosterone levels. Always consult a healthcare professional for personalized advice.
Overall
As a general recommendation, we advise caution regarding cellular alchemy. While it shows promise for testosterone restoration, it remains experimental. Consult a healthcare professional before considering it. For bodybuilders, natural alternatives (like lifestyle changes and supplements) are safer and more widely applicable.
Also Read: Meet the World’s Strongest Grannies
Hormonal balance is a bodybuilder's cornerstone, particularly when PEDs are introduced at supraphysiological levels. Testosterone Cypionate and Primobolan are often combined for muscle growth, strength, and physique refinement. Yet, beyond the anabolic benefits, these compounds exert complex influences on estrogen metabolism—specifically estradiol (E2), a hormone essential for joint health, mood stability, and cardiovascular function. While excessive estrogen can lead to water retention and gynecomastia, insufficient levels may compromise recovery, bone density, and overall well-being. This article explores the question: Is estradiol too low when using high-dose testosterone alongside Primobolan? By examining the physiological mechanisms, potential risks, and evidence-based strategies, we aim to provide insights that encourage informed decision-making. The goal is not to glorify extreme dosing, but to highlight the importance of monitoring, moderation, and health-first practices in bodybuilding.

Check Out 1-Test Cyp 100 by Nakon Medical
A Sneak Peek Into Estradiol
Estradiol (E2), the primary form of estrogen in men, is often misunderstood. While testosterone is celebrated as the driver of muscle growth and strength, estradiol plays a crucial supporting role in maintaining overall health and performance. Produced through the aromatization of testosterone, estradiol contributes to bone density, joint lubrication, cardiovascular protection, and even neurological stability. For athletes pushing their bodies with high-dose anabolic protocols, overlooking estradiol can lead to unintended consequences.
Related Article: Anadrol Cycle Benefits, Doses, Alternatives, etc.
Estradiol is sometimes viewed solely as a hormone to suppress, due to its association with water retention, gynecomastia, and bloating. However, excessively low levels can be just as problematic. Symptoms such as joint pain, decreased libido, mood swings, and impaired recovery often emerge when estradiol is suppressed below physiological norms. This balance is particularly delicate in cycles involving compounds like Testosterone Cypionate, which aromatizes readily, and Primobolan, which does not. The combination can skew estrogen regulation, raising questions about whether estradiol levels are being driven too low.
Understanding estradiol’s role requires moving beyond the simplistic “high is bad” mindset. Instead, responsible bodybuilding emphasizes monitoring through bloodwork, recognizing symptoms, and appreciating estradiol’s protective functions. By acknowledging its importance, athletes can better safeguard long-term health while still pursuing physique goals. Estradiol, far from being the enemy, is a vital component of hormonal harmony that supports sustainable progress in bodybuilding.
High-Dose Protocols: Benefits vs. Risks
Combining large amounts of Testosterone Cypionate with moderate Primobolan—remains a controversial practice. Athletes often pursue these regimens to maximize muscle growth, strength, and physique refinement, yet the physiological trade-offs are significant. While supraphysiological dosing can accelerate progress, it also amplifies the risk of hormonal imbalance, cardiovascular strain, and long-term health consequences. Responsible bodybuilding requires weighing the potential benefits against the risks, recognizing that short-term gains may come at the expense of sustainability. Understanding this balance is essential for athletes who aim to optimize performance without compromising their well-being.
| Aspects | Benefits | Potential Risks |
| Muscle Growth | Rapid hypertrophy due to elevated anabolic environment | Increased risk of tendon stress and disproportionate growth |
| Strength Gains | Enhanced power output and training intensity | Greater strain on joints and connective tissue |
| Physique Refinement | Reduced fat mass and improved muscle definition | Possible hormonal imbalance, including suppressed estradiol |
| Recovery | Faster recovery between sessions | Long-term suppression of natural testosterone production |
| Confidence & Motivation | Psychological boost from visible progress | Mood swings, irritability, or depressive symptoms if hormones destabilize |
| Performance Longevity | Short-term peak performance | Elevated cardiovascular risk, liver strain, and potential fertility issues |
Our Recommended Dosages
We frames dosage as a balancing act—not just numbers, but how they translate into health, recovery, and sustainable progress.
Primobolan (Primo) appears to act as a strong aromatase inhibitor (AI) for some individuals, effectively lowering estradiol (E2) levels. At 150mg Primo alongside high-dose Testosterone Cypionate, bloodwork shows free testosterone at 1737 with E2 at 28. While these numbers may feel subjectively “good,” they highlight the delicate interplay between anabolic dosing and estrogen regulation.
See Why A Newbie Needs Electrolytes Like Salt Before, During, and After Training
Six weeks earlier, with a more moderate testosterone dose (200mg/week), free testosterone measured 1200 and E2 was 40—suggesting that higher Primo intake may be suppressing aromatization more aggressively. The question then becomes: should dosages be adjusted to allow estradiol to rise slightly, or is maintaining current levels acceptable given the absence of negative symptoms? Responsible bodybuilding emphasizes individualized responses, careful monitoring, and prioritizing long-term health over chasing trends in “higher E2” preferences.
| Compound | Current Dosage | Observed Effect | Consideration |
| Testosterone Cypionate | 1300mg/week | Free test at 1737 | High anabolic drive; monitor cardiovascular strain |
| Primobolan | 150mg/week | E2 reduced to 28 | Acts as AI; may suppress estradiol too much |
| Estradiol (E2) | 28 (current) vs. 40 (prior) | Lower than baseline | Evaluate symptoms; consider adjusting Primo or supporting E2 |
Overall
Pursuing enhanced performance through anabolic protocols is always a balancing act between progress and health. High doses of testosterone combined with compounds like Primobolan can deliver visible gains, but they also reshape the hormonal landscape in ways that demand careful attention. Estradiol, often overlooked or misunderstood, plays a vital role in maintaining joint integrity, cardiovascular resilience, mood stability, and recovery capacity. Allowing it to drop too low may undermine the very goals athletes are striving for.
The key takeaway is that success should not be measured only by strength or aesthetics, but by how well overall health is preserved along the way. Regular bloodwork, awareness of physical and emotional cues, and a willingness to adjust protocols are essential for sustainable progress. By respecting the role of estradiol and striving for balance rather than extremes, athletes can achieve results that are not only impressive in the short term but also supportive of long‑term well‑being.

Among fitness enthusiasts and bodybuilders alike, one of the most enduring debates centers on whether full-body workouts or split routines deliver the greatest results. For years, the traditional “bro split” — dedicating each day to a single muscle group — has dominated gym culture, promising targeted growth and aesthetic appeal. Yet, as training science and practical experience continue to evolve, full-body workouts have risen as a powerful alternative that challenges this long‑standing convention.
A full-body workout engages all major muscle groups in a single session, typically performed three to four times per week. This style of training emphasizes compound movements such as squats, deadlifts, presses, and rows, which maximize efficiency while stimulating greater hormonal responses and functional strength. Unlike split routines, which often demand five or more days in the gym, full-body training delivers comparable — and often superior — results in less time, making it especially appealing for athletes, professionals, and anyone balancing fitness with a busy lifestyle.
Beyond efficiency, full-body workouts encourage balanced muscular development and reduce the risk of neglecting smaller muscle groups. They also enhance recovery by distributing workload more evenly across the week, while maintaining higher training frequency for each muscle. Research has shown that stimulating muscles multiple times per week can lead to greater hypertrophy compared to once‑a‑week splits, reinforcing the scientific case for this method.
Ultimately, full-body training is not just about saving time; it’s about maximizing results. By prioritizing strength, balance, and sustainability, this approach proves that sometimes less really is more.
Bro Splits
Bro splits, often called “body part splits,” are one of the most popular training styles in bodybuilding. In this approach, each workout session is dedicated to a single muscle group or a pair of related muscles. For example, Monday might be chest day, Tuesday back day, Wednesday legs, Thursday shoulders, and Friday arms. This allows lifters to focus intensely on one area, performing multiple exercises and high volume for that specific muscle.
The appeal of bro splits lies in their specialization. By isolating muscles, trainees can push them to fatigue with targeted exercises, which can be beneficial for advanced bodybuilders seeking aesthetic symmetry and maximum hypertrophy. It also provides psychological satisfaction — the pump and soreness in a specific muscle group can feel rewarding.
However, bro splits often require five or more gym sessions per week, making them time-consuming and less practical for those with busy schedules. They also limit training frequency for each muscle to once per week, which may not align with research suggesting muscles benefit from being stimulated multiple times weekly. While effective for seasoned lifters, bro splits can be inefficient for beginners or those seeking overall strength and balanced development.
Related Article: Tiny Doses, Big Impact: The PED Revolution
Full-Body Training
Full-body training takes a different approach by targeting all major muscle groups in a single workout session. Typically performed three to four times per week, these workouts emphasize compound movements such as squats, deadlifts, bench presses, pull-ups, and overhead presses. Each session delivers a balanced stimulus across the body, ensuring no muscle group is neglected.
The strength of full-body training lies in its efficiency. By working multiple muscles at once, trainees maximize calorie expenditure, hormonal response, and functional strength. This style also increases training frequency for each muscle group — instead of hitting chest once a week, it might be trained three times, leading to greater hypertrophy and strength gains over time. For beginners, athletes, and busy professionals, this method offers a sustainable way to build muscle without living in the gym.
Another advantage is recovery. Because workload is spread across sessions, muscles receive consistent stimulation without excessive fatigue. Full-body training also fosters balanced development, reducing the risk of overemphasizing certain areas while neglecting others. While it may lack the extreme specialization of bro splits, full-body workouts deliver superior overall results for most lifters, proving that training smarter often beats training longer.
Benefits of Full-Body Workouts
Greater Training Frequency – Each muscle group is worked multiple times per week, leading to more consistent stimulation and growth.
Time Efficiency – Fewer gym sessions are needed (3–4 per week vs. 5–6 for splits), making it easier to fit into busy schedules.
Balanced Muscle Development – Ensures no muscle group is neglected, reducing imbalances common in split routines.
Improved Recovery – Workload is spread across sessions, preventing excessive fatigue in one muscle group.
Higher Calorie Burn – Compound lifts involving multiple muscles increase energy expenditure, aiding fat loss.
Functional Strength Gains – Focus on compound movements builds strength that translates better to real-life activities.
Hormonal Advantage – Large, multi-joint exercises trigger stronger anabolic responses (testosterone, growth hormone).
Flexibility & Consistency – Missing a workout doesn’t derail progress since each session covers the whole body.
Beginner-Friendly – Simpler structure helps newcomers learn proper technique and progress faster.
Sustainability – Easier to maintain long-term, reducing burnout compared to high-volume split routines.
Supplement Alternatives to Bro-Splits
Instead of relying on bro splits, athletes can support full-body training with dietary strategies and supplements that enhance recovery, muscle growth, and overall performance. The focus shifts from isolating muscles to fueling the entire body consistently.
Check: Top Fitness Games to Play in 2026
Protein Supplements
- Whey Protein: Fast-digesting, ideal post-workout for muscle repair.
- Casein Protein: Slow-digesting, supports overnight recovery.
- Plant-Based Protein: Pea, rice, or soy protein for those avoiding dairy.
Creatine Monohydrate
- Boosts strength and power output.
- Supports repeated high-intensity efforts across compound lifts.
Branched-Chain Amino Acids (BCAAs)
- Helps reduce muscle soreness.
- Supports recovery when training multiple muscle groups in one session.
Essential Amino Acids (EAAs)
- More complete than BCAAs, ensuring protein synthesis is maximized.
Beta-Alanine
- Delays muscle fatigue by buffering lactic acid.
- Useful for longer full-body sessions with compound lifts.
Omega-3 Fatty Acids
- Anti-inflammatory properties aid recovery.
- Supports joint health under heavy compound training.
Multivitamins & Minerals
- Covers nutritional gaps.
- Important for energy metabolism and muscle function.
Carbohydrate Supplements
- Dextrose or maltodextrin for quick glycogen replenishment post-workout.
- Helps sustain energy during demanding full-body sessions.
Caffeine
- Enhances focus and endurance.
- Useful for maintaining intensity across longer workouts.
Hydration & Electrolytes
- Sodium, potassium, magnesium to prevent cramps.
- Critical for full-body routines that tax multiple systems at once.
Must Read: Comparing Muscle Hardness and Size
Overall
The debate between full-body workouts and split routines has long shaped the way athletes and bodybuilders approach their training. While bro splits offer targeted intensity and aesthetic appeal, full-body training demonstrates clear advantages in efficiency, balance, and long-term sustainability. By engaging all major muscle groups in each session, lifters maximize their time in the gym, stimulate greater hormonal responses, and build functional strength that extends beyond appearance.

Buy Semaglutide by Deus Medical
Research consistently shows that muscles benefit from being trained multiple times per week, a principle that full-body workouts naturally embrace. This higher frequency not only accelerates hypertrophy but also fosters improved recovery and reduces the risk of overtraining specific muscle groups. For beginners, athletes, and busy professionals, the simplicity and practicality of full-body routines make them an accessible yet powerful option. Even seasoned lifters can benefit from incorporating full-body sessions to break plateaus and restore balance.
Ultimately, the choice of training style should align with individual goals, but the evidence is clear: full-body workouts provide a comprehensive, efficient, and effective path to strength and muscle growth. By prioritizing smart training over sheer volume, lifters can achieve lasting results and prove that sometimes, less truly is more.
Energy is the foundation of every workout. Whether you’re grinding through heavy sets, pushing past fatigue on the treadmill, or chasing that last rep, your body’s ability to generate and sustain power determines how far you can go. At the heart of this process are mitochondria—the microscopic engines inside muscle cells that convert nutrients into usable energy. These tiny structures don’t just keep you moving; they influence endurance, recovery, and even muscle growth.
Training isn’t only about building bigger muscles—it’s about optimizing the machinery that fuels them. Exercise stimulates mitochondrial biogenesis, the creation of new mitochondria, which enhances energy production and metabolic efficiency. For fitness athletes and bodybuilders, this means longer-lasting strength during workouts, improved recovery between sets, and the ability to tap into both carbohydrates and fats for fuel. Stronger mitochondria help delay fatigue, sharpen focus, and support lean muscle development by ensuring nutrients are used effectively.
But the path to stronger mitochondria goes beyond the gym floor. Nutrition rich in antioxidants, adequate protein intake, quality sleep, and stress management all play vital roles in protecting and enhancing these cellular engines. When combined with smart training strategies—whether endurance cardio, high-intensity intervals, or resistance work—these lifestyle factors create a powerful synergy that elevates performance.
Mitochondria and Muscle Hypertrophy
When it comes to bodybuilding, most people think about lifting heavier weights, eating more protein, and pushing for progressive overload. Yet beneath the surface of every rep lies a cellular powerhouse that makes hypertrophy possible: the mitochondria. These tiny organelles are responsible for producing adenosine triphosphate (ATP), the energy currency that fuels muscle contractions. Without efficient mitochondria, even the most disciplined training program stalls because the body cannot sustain the energy demands required for growth.
Muscle hypertrophy—the enlargement of muscle fibers—depends on repeated cycles of stress, recovery, and adaptation. During intense resistance training, mitochondria ramp up ATP production to meet the immediate energy needs of contracting fibers. But their role doesn’t end there. Post-workout, mitochondria help regulate recovery by supporting protein synthesis, repairing damaged tissue, and clearing metabolic byproducts such as lactate. This recovery process is critical: hypertrophy occurs not during the workout itself, but in the rebuilding phase that follows.
Related Article: Top 7 Superfoods For Building Muscle Mass
Stronger, more numerous mitochondria also improve muscular endurance. While hypertrophy is primarily driven by mechanical tension and metabolic stress, the ability to sustain higher training volumes without premature fatigue allows bodybuilders to push harder and longer. Enhanced mitochondrial density means better oxygen utilization and fat oxidation, which reduces reliance on glycogen alone. This balance helps athletes maintain lean mass while minimizing fat accumulation—a key goal in bodybuilding aesthetics.
Training methods such as high-intensity interval training (HIIT), moderate-intensity “Zone 2” cardio, and metabolic conditioning can complement heavy lifting by stimulating mitochondrial biogenesis. When combined with proper nutrition—adequate protein, micronutrients like magnesium, and mitochondrial-supportive compounds such as CoQ10—bodybuilders create an internal environment where energy production and muscle growth work hand in hand.

Generally, hypertrophy isn’t just about lifting weights; it’s about empowering the cellular engines that make growth possible. By strengthening mitochondria, bodybuilders unlock greater energy, faster recovery, and more sustainable muscle gains.
Must Read: Primal Movements: Our Ultimate Guide for Maximum Results
Strength vs. Endurance Balance
Bodybuilding is often associated with heavy weights, low repetitions, and the pursuit of maximum muscle size. Yet, the balance between strength and endurance training plays a critical role in optimizing performance and long-term gains. While strength training primarily targets muscle hypertrophy through mechanical tension and progressive overload, endurance training enhances mitochondrial density and efficiency, ensuring that muscles can sustain effort and recover more effectively.
Strength-focused workouts rely heavily on anaerobic energy systems, which deliver quick bursts of ATP but also generate metabolic byproducts that contribute to fatigue. Without a strong aerobic foundation, bodybuilders may struggle with recovery between sets or find themselves limited in training volume. Endurance training, particularly at moderate intensities, strengthens the aerobic system by improving oxygen utilization and fat oxidation. This not only supports longer workouts but also helps maintain a leaner physique by reducing reliance on glycogen alone.
The key lies in integration rather than choosing one over the other. Incorporating short bouts of high-intensity interval training (HIIT) or steady-state cardio alongside resistance training can stimulate mitochondrial biogenesis without compromising muscle growth. Periodization strategies—alternating phases of strength emphasis with endurance conditioning—allow athletes to maximize hypertrophy while building resilience.
Ultimately, the balance between strength and endurance ensures that bodybuilders are not just bigger, but also more efficient, better recovered, and metabolically healthier. By training both systems, athletes unlock the full potential of their muscles, combining raw power with sustained energy for superior performance.
Recovery and Reduced Fatigue
Progress is built not just in the gym but in the hours that follow. Recovery is where muscle fibers repair, adapt, and grow stronger. Mitochondria play a central role in this process by managing energy availability and clearing metabolic waste, which directly impacts how quickly athletes bounce back from intense training.
During heavy lifting, muscles rely on anaerobic energy pathways, producing lactate as a byproduct. Accumulation of lactate and hydrogen ions contributes to the familiar “burn” and eventual fatigue. Well-trained mitochondria help buffer and recycle these metabolites, converting lactate back into usable energy through oxidative pathways. This reduces soreness and allows bodybuilders to recover faster between sets and sessions.
Efficient mitochondria also support protein synthesis during recovery. By generating ATP consistently, they provide the energy needed for repairing microtears in muscle fibers and building new tissue. This means that athletes with stronger mitochondrial function can sustain higher training volumes without compromising recovery quality.
Beyond the cellular level, improved mitochondrial capacity enhances overall resilience. Better oxygen utilization and fat oxidation reduce reliance on glycogen, sparing muscle energy stores and minimizing exhaustion. This translates into steadier performance across long workouts and quicker readiness for the next session.
Integrating endurance-based conditioning, adequate sleep, and nutrient support—such as antioxidants and omega-3 fatty acids—further boosts mitochondrial recovery pathways. For bodybuilders, this synergy means less downtime, reduced fatigue, and more consistent gains. In essence, mitochondria are the silent partners ensuring that every rep pays off long after the workout ends.
Fat Utilization and Lean Physique
Achieving a lean and defined physique is just as important as building muscle mass. While resistance training drives hypertrophy, the efficiency of mitochondria determines how effectively the body utilizes fat as a fuel source. Stronger mitochondria enhance oxidative metabolism, allowing muscles to burn fat more readily during both exercise and rest. This shift toward fat oxidation not only spares glycogen for high-intensity efforts but also supports the reduction of excess body fat, leading to sharper muscle definition.
When mitochondrial function is optimized, the body becomes more metabolically flexible—able to switch between carbohydrate and fat fuel sources depending on the demands of training. This flexibility is crucial during cutting phases, where athletes aim to preserve muscle while shedding fat. By relying more on fat oxidation, bodybuilders can maintain energy levels without compromising lean tissue.
Training methods such as Zone 2 cardio (moderate-intensity sessions that maximize fat burning) and metabolic conditioning workouts stimulate mitochondrial biogenesis, expanding the body’s capacity to use fat efficiently. Combined with strength training, these approaches create a dual benefit: muscle growth supported by resistance work and fat reduction driven by improved mitochondrial function.
Nutrition also plays a key role. Diets rich in healthy fats (omega-3s, monounsaturated fats), adequate protein, and micronutrients like iron and B vitamins support mitochondrial enzymes involved in fat metabolism. Together, these strategies ensure that bodybuilders not only build size but also sculpt a physique that is lean, defined, and competition-ready.
Training Techniques that Promote Mitochondria Growth
While bodybuilding traditionally emphasizes heavy resistance training for hypertrophy, incorporating specific techniques that stimulate mitochondrial growth can significantly enhance performance, recovery, and physique. Mitochondria thrive under metabolic stress, and certain training modalities are particularly effective at driving adaptations that increase both their number and efficiency.
High-Intensity Interval Training (HIIT): Short bursts of maximal effort followed by recovery periods challenge the body’s energy systems, forcing mitochondria to adapt. For bodybuilders, adding one or two HIIT sessions per week can improve endurance and accelerate fat oxidation without compromising muscle mass.
Zone 2 Cardio: Moderate-intensity aerobic training—often performed at a pace where conversation is possible—maximizes fat utilization and stimulates mitochondrial biogenesis. This type of cardio complements strength training by building a strong aerobic base, improving recovery between sets, and supporting lean muscle preservation during cutting phases.
Metabolic Conditioning (MetCon): Circuits that combine resistance and cardio elements push both anaerobic and aerobic systems simultaneously. These workouts elevate heart rate, increase lactate clearance, and drive mitochondrial adaptations while maintaining a bodybuilding focus on muscle engagement.
Periodization Strategies: Alternating phases of heavy lifting with endurance or conditioning blocks ensures balanced development. This approach prevents overtraining, maintains hypertrophy, and steadily builds mitochondrial resilience.
By blending these techniques with traditional bodybuilding routines, athletes create a training environment that not only builds muscle size but also strengthens the cellular engines powering growth. The result is a physique that is not only bigger and stronger but also more efficient, lean, and sustainable over time.
See: The Ultimate Fitness Apps
Nutrition Synergy
Training alone cannot maximize mitochondrial growth—nutrition plays an equally vital role in bodybuilding performance and physique. Mitochondria rely on a steady supply of nutrients to generate ATP, repair muscle tissue, and regulate metabolic processes. When diet and training work in synergy, bodybuilders create the optimal environment for both hypertrophy and cellular energy efficiency.
Protein and Amino Acids: Adequate protein intake is essential for muscle repair and growth, but amino acids also support mitochondrial enzymes involved in energy metabolism. Branched-chain amino acids (BCAAs) and leucine, in particular, help stimulate protein synthesis while fueling recovery.
Healthy Fats: Omega-3 fatty acids and monounsaturated fats enhance mitochondrial membrane fluidity, improving efficiency in energy transfer. These fats also reduce inflammation, supporting faster recovery and lean muscle preservation.
Micronutrients: Vitamins and minerals such as magnesium, iron, and B vitamins are critical cofactors in mitochondrial energy pathways. Iron supports oxygen transport, while magnesium aids ATP production. Deficiencies in these nutrients can impair both performance and recovery.
Antioxidants: Intense training generates oxidative stress, which can damage mitochondria. Nutrients like vitamin C, vitamin E, and compounds such as CoQ10 help neutralize free radicals, protecting mitochondrial integrity and sustaining long-term function.
Timing and Balance: Strategic nutrient timing—protein post-workout, carbohydrates to replenish glycogen, and fats for sustained energy—ensures mitochondria have the resources they need at the right moments.
By aligning nutrition with training, bodybuilders not only fuel muscle growth but also strengthen the cellular engines that power every rep, set, and recovery phase. This synergy is the foundation of sustainable gains and a lean, defined physique.
Overall
Mitochondria may be invisible to the eye, but their impact on bodybuilding is undeniable. They are the engines that power every rep, every set, and every recovery phase. By strengthening mitochondrial function, athletes unlock more than just energy—they gain the ability to train harder, recover faster, and sculpt a leaner, more resilient physique.
We’ve discussed how mitochondria influence muscle hypertrophy, balance strength with endurance, reduce fatigue, and enhance fat utilization. We’ve also explored training techniques and nutritional strategies that directly support mitochondrial growth. Together, these elements highlight a simple truth: bodybuilding is not only about building bigger muscles, but also about optimizing the cellular machinery that makes growth sustainable.
The path to long-term success lies in synergy—combining heavy lifting with conditioning, fueling the body with the right nutrients, and respecting recovery. When mitochondria are nurtured, they transform the body into a more efficient, powerful, and enduring system.
In the end, focusing on mitochondrial health is about more than performance—it’s about longevity. Stronger mitochondria mean stronger muscles, but they also mean a stronger athlete overall. By fueling energy from within, bodybuilders can push past limits, achieve peak aesthetics, and sustain their gains for years to come.


Too Low Estradiol? Insights from High-Dose Testosterone and Primobolan Use

From Cholesterol to Cortisol: The Molecular Story of Steroids

One Workout to Rule Them All: Full-Body Training Over Splits

Fueling Energy from Within: How to Build Stronger Mitochondria Through Training

Is Training/Lifting Barefoot A Good Idea? Find Out

Using Insulin Needles to Inject AAS: Pros and Cons

Is NAD+ The Best Anti-aging Molecule for Men Over 40?

Estrogen Management: SERMs and AIs Compared

The Testosterone Trap: Why Bigger Levels Don’t Guarantee Bigger Muscles

Sodium, Potassium, and Pump: The Science Behind Electrolytes Balance in Bodybuilding
Sodium, Potassium, and Pump: The Science Behind Electrolytes Balance in Bodybuilding
Estrogen Management: SERMs and AIs Compared
Using Insulin Needles to Inject AAS: Pros and Cons
The Testosterone Trap: Why Bigger Levels Don’t Guarantee Bigger Muscles
Is NAD+ The Best Anti-aging Molecule for Men Over 40?
Is Training/Lifting Barefoot A Good Idea? Find Out
Fueling Energy from Within: How to Build Stronger Mitochondria Through Training
One Workout to Rule Them All: Full-Body Training Over Splits
From Cholesterol to Cortisol: The Molecular Story of Steroids
Too Low Estradiol? Insights from High-Dose Testosterone and Primobolan Use
Sodium, Potassium, and Pump: The Science Behind Electrolytes Balance in Bodybuilding
Estrogen Management: SERMs and AIs Compared
Using Insulin Needles to Inject AAS: Pros and Cons
The Testosterone Trap: Why Bigger Levels Don’t Guarantee Bigger Muscles
Is NAD+ The Best Anti-aging Molecule for Men Over 40?
Is Training/Lifting Barefoot A Good Idea? Find Out
Fueling Energy from Within: How to Build Stronger Mitochondria Through Training
One Workout to Rule Them All: Full-Body Training Over Splits
From Cholesterol to Cortisol: The Molecular Story of Steroids
Too Low Estradiol? Insights from High-Dose Testosterone and Primobolan Use
-

 Bodybuilding Products2 years ago
Bodybuilding Products2 years agoTelmisartan In Bodybuilding: An Expert’s Advice
-
 Steroids2 years ago
Steroids2 years agoAnadrol Cycle: Benefits, Doses, Alternatives, etc.
-

 Anabolic Steroids2 years ago
Anabolic Steroids2 years agoJoint Stiffness: How to Manage It While on AAS
-
 Bodybuilding1 year ago
Bodybuilding1 year agoPrimal Movements: Our Ultimate Guide for Maximum Results
-
 Bodybuilding1 year ago
Bodybuilding1 year agoHow Effective is Bone Broth for Recovery?
-
 Steroids1 year ago
Steroids1 year agoBodybuilder Winter Clothing: Staying Warm and Stylish
-
 Steroids2 years ago
Steroids2 years agoOmnitope (Oxytocin)
-
 Bodybuilding2 years ago
Bodybuilding2 years agoHow Much Is Too Much Cardio? Understanding Heart Rate Zones
-

 Steroids1 year ago
Steroids1 year agoSleeping Positions for Effective Muscle Recovery
-
 Steroids1 year ago
Steroids1 year agoOstarine For Beginners: The Ultimate Guide
-
 Bodybuilding1 year ago
Bodybuilding1 year ago2nd Edition of Natural Bodybuilding Competition Facts
-
 Bodybuilding1 year ago
Bodybuilding1 year agoAre Nootropics a Better Option to AAS?
-
 Bodybuilding1 year ago
Bodybuilding1 year agoTop Video Games for Bodybuilders in 2025
-
 Steroids11 months ago
Steroids11 months agoRaloxifene (Evista) 101: A Non-Surgical Solution for Gyno
-
 Bodybuilding2 years ago
Bodybuilding2 years agoDemystifying Hypertrophy Training
-
 Steroids1 year ago
Steroids1 year agoTips on How to Store Peptides and HGH
-
 Steroids12 months ago
Steroids12 months agoWhy Post-Cycle Therapy (PCT) Fails After a Nandrolone Cycle
-

 Beginners1 year ago
Beginners1 year ago14 Morning Run Safety Tips for Bodybuilding and Fitness
-
 Steroids10 months ago
Steroids10 months agoCreatine vs Myostatin: An Expert’s Analysis
-
 Steroids1 year ago
Steroids1 year agoGlutathione – The Most Underrated Antioxidant
-
 Bodybuilding2 years ago
Bodybuilding2 years agoList of FDA-Approved Peptides
-

 Product Reviews2 years ago
Product Reviews2 years agoTop Vitamins for Skin Health
-
 Anabolic Steroids2 years ago
Anabolic Steroids2 years agoHow Much Do You Know About B-AET? A Fat Burner You’ve Been Missing
-

 Bodybuilding2 years ago
Bodybuilding2 years agoHormone Replacement Therapy (TRT) Cycle Guide
-

 Anabolic Steroids2 years ago
Anabolic Steroids2 years agoAnavar Cycle for Men and Women